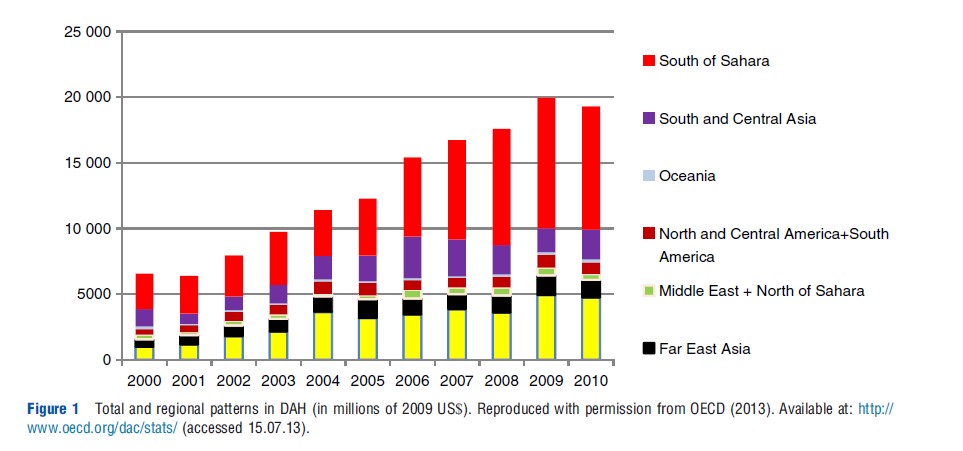
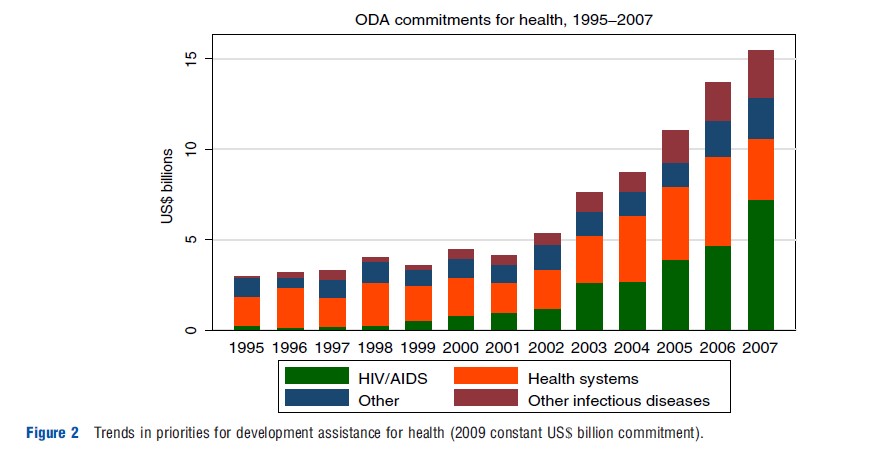
In 1990, development assistance for health (DAH) flowing from the Organization of Economic Cooperation and Development (OECD) countries amounted to only US$4 billon accounted in the index year of 2009. This figure had increased to US$19 billion by 2010, although the year 2009 saw a decline in DAH perhaps due to the economic downturn in the developed countries. Figure 1 shows the dramatic increase since 2000. Although much of it can be due to the commitment to combat human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS) epidemics, the overall increase is substantial, and there has been recognition of other health care issues as well, as shown in Figure 2. Naturally, questions have risen as to the effectiveness of development assistance for health. Of course, the pathways through which one can examine whether aid has contributed to improved health are extremely difficult to discern. This is one of the issues addressed below. A substantial number of intermediary issues have been examined in the literature. Among the important issues concerning the pathways are what has been recognized as fungibility, coordination, and fragmentation. After a brief description on flow of development assistance for health (DAH), the authors ascertain the current thinking on aid effectiveness.
Trends In Development Assistance for Health
Of the US$127 billion distributed in overseas development assistance (ODA) in 2009 from OECD-DAC, approximately 16% (19 billion) was directed toward health; the corresponding figure for the sub-Saharan Africa (SSA) is 44% (US$12 billion of US$26.7 billion ODA). Thus, health issues play a prominent role in the total development assistance where poverty issues loom large. The prominence of recognition of HIV/AIDS as a global problem resulted in a proportion of DAH going to HIV/AIDS, rising from being approximately 10% of the total amount DAH in 2000 to nearly 40% by 2007 (see Figure 2). Perhaps, due to this crisis there have been proliferations of other actors such as private foundation, global health partnership, and NGOs toward ensuring greater DAH. Once these mechanisms have been taken into account, estimation of total DAH can rise by 20–30%.
Given that for some countries development assistance for health can amount to a large proportion of the public health budget, the modality of funding is an important issue. A useful literature that feeds into analysis of aid-effectiveness is the examination of the wide variety of funding modalities, which depend on the amount of earmarking for specific usage and the extent to which the myriad of actors rely on government systems for planning, disbursement, and monitoring of funds. The myriad of modalities include direct funding of projects, program aid, sector-wide approaches, and budget support, with projects having the most earmarking and budget support the least. A more recent form of aid giving has been through direct NGO funding. Discerning these channels from the existing data sets has been difficult. At least one study concludes that aid modalities independent of government may induce greater commitment of funding toward health improvement from the government. Although one can take account of a certain degree of endogeneity from the fact that the recipient country’s governance structure influences the method through which aid is delivered, these results do not prove conclusive. Knack notes that the use of country infrastructure by the donors is related to (1) donor’s share of aid provided to the recipient, (2) perception of corruption in the recipient country, and (3) the public support for aid in the donor country. The perception of corruption in aid has been tied to the issues regarding fungibility. Another concern has been that aid is provided through multiple transfer instances what one may label as aid events; and for a single country there are multiple donors as indicated already. There are two concerns underlying here: firstly that aid giving involves multiple episodes of transactions between the donors and the recipients; and secondly that there may be too many aid givers. These two issues have been recognized as aid fragmentation, perhaps stemming from lack of coordination among donors.
As ODA can be specified to be used only for developmental use as opposed to military use, within the developmental budget, there is, of course, a mandate as to what can be funded, such as health and education. Various modes have been used to mandate that the health budget have to provide for both specific and general use. One mode of delivery is to offer through basket funding to the government’s nonmilitary budget; this has little or no earmarking. A widely used method is called the sector-wide approach (popularly known as SWAP) which can be described as a coordination mechanism for donors working on the same sector. It is a form of budget support where funding is more targeted. Program-based approach has gained prominence; they are characterized by having a single comprehensive program and budget framework, donor coordination in budgeting procedures, management, procurement and reporting. In recent years, nearly exclusive to funding health problems in developing countries are the global health initiatives, which are vertical programs to tackle a single public health issue through a consortium of ODA and private funding.
Effectiveness of ODA is a much discussed recent topic in the economics literature, although initial literature dates back to Pack and Pack in 1983 when much of ODA may have been driven by geopolitical concerns; and there were essentially two donors. The geopolitical nature of aid giving induces Rajan and Subramanian, for example in their now well-known paper, to leave out Egypt.
Measuring Effectiveness Of Development Assistance for Health
The unambiguous conclusion from the empirical literature on aid effectiveness as stated by Bourguignon and Sundberg is that it has ‘yielded unclear and ambiguous results.’ They also state that this should not be a surprise given the politics of aid with the heterogeneity of motives; and more importantly, the complex causality chain linking external aid to final outcomes. For ODA, one of the most important outcome measures of development has been growth rate. Ignoring the mechanism through which ODA may affect the growth rate, a set of oftquoted studies using reduced form equations have estimated the impact on growth rate to get results that indicate that the relationship between aid and development outcomes is fragile and often ambiguous. The results are slightly more optimistic when some form of mechanism through which aid can affect growth rate has been taken into account. For example, Arndt and coauthors show a positive impact of ODA on growth through a structural model where life expectancy along with investment and education are intermediary factors through which aid affects growth.
The use of reduced form approaches have prevailed in showing the impact of development assistance for health. DAH is, of course, intended for improving health in most cases. It is also part of the developmental aid as opposed to the military or the politically motivated assistance. Clements and coauthors have indicated that for the short run aid allocated to support budget and balance of payments commitments and infrastructure result in rising income. They speculate that aid promoting democracy, health, and education will have a long run impact on growth. Minoiu and Reddy have shown through a Gaussian Mixture Model that developmental aid contributes to growth, whereas the same cannot be said of nondevelopmental aid. Burnside and Dollar conclude that ODA equivalent to 1% of GDP in the recipient country reduces child mortality by 0.9%. Mishra and Newhouse have shown through a Generalized Method of Moments estimation for data from 1975 to 2004 that doubling per-capita health aid decreases infant mortality by 2% for the subsequent five-year period. Earlier, Peck and Peck had showed statistically insignificant results for infant mortality rate.
As mentioned, the mechanism through which aid can improve an outcome is too complex, and simply answering whether an outcome is achieved or not is not very helpful especially if the answer is that the outcome of interest does not seem to have a desirable relationship with ODA. One way to discern pathways through which ODA may or may not work is to ask questions as to whether elements of an economy that ODA funds make for sound policy-making. This may involve macroeconomic analyses or an impact evaluation of projects. It is not possible to evaluate all projects; it is certainly not possible to list all projects that may have used DAH wisely in this monograph. Given the nature of implementation of projects, it is also likely to be misled to list successful projects to be applied from places and times different from the original situation in which they were placed.
The general structure of aid giving is likely to have played a significant role in achieving the outcome which the authors finally arrive at. Many ODA was distributed through conditionality which may have resulted in binding policy makers around donor priorities to ensure policy compliance and implementation. The Paris Declaration on Aid Effectiveness adopted in March 2005, with 100 country signatories, recommended improving aid coordination, promoting donor alignment with country strategies, and cutting the ‘compliance burden’. Examining the methods through which ODA have been delivered and the intermediary processes it may engender can help us to understand whether ODA would be effective or not. In doing so, it is not emphasized on private philanthropy which is already engaged in development project funding in a significant way, especially in aiming to improve health. Private philanthropy should not be considered as DAH as for some countries it is also domestic fund; and secondly the rules governing such funding are entirely different from that of ODA funding.
Factors Affecting The Effectiveness Of Development Assistance for Health
Clearly a factor that would affect aid effectiveness is whether or not it goes to the right place; that is, do the poorest people of the world receive development assistance for health. Secondly, given that some of the DAH is targeted toward particular activities, are these in some ways the right activities that should be funded? It is then turned to a more subtle point of aid architecture or process factors that might be affecting how well DAH is able to improve health: predictability, fragmentation, and fungibility. Finally, some important elements that motivate the actions of the players involved in making aid more effective are noted.
Funding The Poor
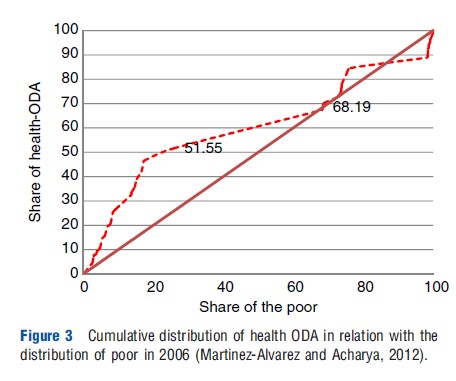
Given that the countries of SSA, the poorest region to which aid flows, have received a large share of foreign aid in terms of DAH, the aim of development assistance to generate human development perhaps is likely to have been met. Despite the published results of a cross-country analysis that found no correlation between countries’ GDP per capita and the amount of DAH they received, although this is improving, in terms of per-capita DAH is indeed aimed toward poorer countries. Although in terms of total aid the amount of DAH or ODA is aimed at the country which has the largest number of poor – India, as it is a middle income country, it receives a very low-level of per-capita DAH. Distribution of DAH is fairly consistent with the motive of aiding the poor in the poorest country. Figure 3 shows the relationship between the cumulative proportion of poor (defined as living under US$1 a day) and the cumulative amount of DAH distributed for 56 countries, including India and China, but excluding countries with a population smaller than one million and those for which DAH made up for less than 1% of their total government budget. These countries were ranked by per-capita income, averaged over 1995–2006. For this sample of countries, the first 25 countries amounted to containing 26% of the total poor, whereas the amount of health ODA going to these countries amounted to 51.5% of the total amount of aid in our sample. Of these countries, 22 were in SSA. In some countries DAH does nearly make up for the entire public sector health budget and this may perhaps lead to aid dependency.
Funding Illnesses
As funding can be earmarked, it is important to know how it is earmarked. One way to measure the impact is to see how the burden of illness matches funding. A commonly used measure is disability-adjusted life years (DALYs) for burden. Nugent has shown that while US$0.78 per DALY is allocated toward combating noncommunicable diseases in 2007, US$23.9 per DALY was allocated to HIV/AIDS, Malaria, and tuberculosis. However, a bulk of the latter funding was targeted toward combating HIV/AIDS. Of the US$13.8 DAH that could be accounted for by Ravishankar and coauthors, US$4.9 was spent on HIV/AIDS, compared with US$0.6 billion spent on tuberculosis; the corresponding numbers for malaria and health system were US$0.7 billion and US$0.9 billion. More funding is allocated toward drugs than to human infrastructure.
Predictability
For donor countries, ODA is discretionary spending without the backing of any electoral constituency that needs to be placated through political seigniorage. Predictability in regard to ODA is defined by OECD as (1) long-term consistency and (2) disbursement of committed funds in a timely manner. A panel regression of data from 60 low-income countries from the time period of 1990–2005 found that annually there was a great deal of differences between disbursements and commitments, particularly in SSA and the time trend did not show an improvement. Some of this discrepancy can be attributed to a lack of stability in the recipient country. However, the larger reasons for the discrepancy may well be due to the unmet policy conditions by the recipients, donor administrative and political problems. A lack of consistency in funding availability hinders planning for the long term and may force adjustments and changes to original budget plans in the recipient country.
Fragmentation
An increased level of development funding has resulted in the proliferation in the number of donors as well the number of transactions that mobilize the funding processes. Frot and Santiso found Tanzania, a poor stable democracy, had 1601 aid projects in 2007, although the attraction of Tanzania may be due to its stronger institutions. Acharya and coauthors note that fragmentation causes direct transaction costs both to the total aid budget and the recipient country; further, it exacerbates skill shortage in the recipient country by diverting management attentiveness. Anderson shows through econometric techniques that fragmentation does impose administrative costs. Fragmentation may lead to duplication of projects and repetitive activities. Mueller and coauthors have observed that there is great many similar types of training for health workers in Malawi. As fragmentation can be due to the presence of increasing number of donors, Knack and Rahman have emphasized that bearing of responsibilities of outcome of developmental funding can be diluted. Individual country will be less able to claim credit for success; and the result may be that fear of free-ridership induces a lack of effort on the part of donor countries. Fragmentation may also limit economies of scale as project expansion may be limited by the donor’s budget ceilings. Principally, the 2005 Paris declaration may have been aimed at fragmentation; 100 countries have recognized that improving aid coordination and promoting alignment with country strategies is a big step toward making ODA more effective.
Fungibility
Fungibility centers around the possibility that ODA becomes a substitute for developmental expenditure that recipient countries are willing to undertake rather than complement the government’s developmental budget. It has also become synonymous with corruption. However, fungibility can be seen to be a rational response to sectoral earmarked funds. It also signals that the donor and recipients may have different priorities. One way that a finance ministry can see any type of ODA is to view it as extra revenue. Naturally, for a particular sector the recipient countries would increase the total expenditure in that sector; it may or may not maintain or increase its funding from its own revenue. However, among some policymakers there seems to be an expectation that any increase in DAH should not reduce any domestic expenditure. The response in the academic literature has been very different than policy makers. The academic literature sees fungibility as an extension of the literature on centralized allocation under a federalized system. Economists generally would be surprised by the fact that the local expenditure actually exceeds what would be predicted by the income effect of additional revenue allocated from the central government. Estimates of the extent of fungibility in the health sector for every dollar allocated through DAH on average to a country vary from a decrease in US$0.27–1.65 to a US$1.50 increase. These results depend on the methodologies used including how the dependent variable of total domestic expenditure is calculated. Some factors can be associated with increased fungibility; these include low-levels of GDP per capita of the recipient, fragmentation, and lack of predictability of DAH flow. From a fiscal point of view, the optimal response to lack of reliability of ODA flow is to smooth DAH by spreading it across different years, a practice advised by the IMF.
Motivations And Relations
The issue of fungibility highlights the fact that as economic agents donors and recipients are likely to have different motives. Donors may well be monolithic in their home political structures but by no means in their home country’s attitude toward ODA; and the recipient make up for divergent types of governments ranging from those that are war torn to those that have experienced more or less stable democracy since independence. The donors are accountable to their government and domestic public opinion. The recipients stand in relation perhaps to fill the revenue gap for funds needed for developmental project.
As Knack and others have pointed out, the number of donors shapes donor incentives where development can be seen as a public good which is likely to result in donors eluding individual responsibility. The equivalence of Niskanen type of rational bureaucracy on the donor’s part may well be toward spending of funds rather than achieving results where the links from funds to outcome may be tenuous. This has come to be known as ‘money-moving syndrome.’ The consistency between the donor government’s motives and development also plays a role. One must also note that the governments of the recipient countries may have different developmental interest or may even have little interest beyond remaining in power. The relation between the donor and the recipient can be understood as something similar to the canonical principal–agent relationship. The donor is not able to judge or monitor the recipient’s commitment to development the way that may have been agreed. The donor stands in relation as the principal who may wish for outcomes which can only be achieved by the recipient, the agent. Usual aid practices ignore this fact and unenforceable conditionalities have been usually implemented. Bourguignon and Sunderberg recommend that the aid recipient be free to choose development policies and to implement them and that aid should be ‘‘made dependent on observed or possibly foreseeable progress in development outcomes like poverty reduction, improved literacy rates, lower child mortality, etc., and on the observable general quality of policies.’’
Discussion
What can be highlighted here is that effectiveness of DAH measured in terms of outcome is inconclusive; but most likely DAH along with ODA has not resulted in very significant changes in health outcomes. The key factors affecting the impact of aid on the development that are emphasized here are allocation of resources, donor fragmentation, fungibility of funding, and issues related to making the recipient accountable. That the auhors are unable to gauge the performance of ODA or DAH clearly does not entail that assistance to poor countries should be stopped or even drastically curtailed. Further, political expediency is not likely to move toward such a situation. Thus, making aid effective is a priority for many countries.
Where the link between outcomes and DAH would always be statistically questionable, for ODA relation to be based on performance one would need to examine factors such as governance, country practices, and the outcome results that are observables or can be monitored. An examination of smallscale programs will be valuable toward determining a set of best practices. For successful scaling up of best practices, as has been noted by Medlin and coauthors, the important factors are country ownership, strong leadership and management, and realistic financing.
References:
- Acharya, A., Fuzzo de Lima, A. T. and Moore, M. (2006). Proliferation and fragmentation: Transaction costs and the value of aid. Journal of Development Studies 42, 1–21.
- Anderson, E. (2011) Aid fragmentation and donor transaction costs. Working Paper 31. UEA, UK: School of International Development.
- Arndt, C., Jones S. and Tarp, F. (2011). Aid effectiveness: Opening the black box. UNU-WIDER Working Paper No. 2011/44. Helsinki: UNU-WIDER.
- Banerjee, A. (2006). Making aid work: How to fight global poverty effectively. Working paper. Cambridge, MA, USA: MIT, Economics Department.
- Bourguignon, F. and Sundberg, M. (2007). Aid effectiveness – Opening the black box. American Economic Review 97, 316–321.
- Burnside, C. and Dollar, D. (2000). Aid, policies, and growth. American Economic Review 90(4), 847–868.
- Celasun, O. and Walliser, J. (2008). Predictability of aid: Do fickle donors undermine aid effectiveness? Economic Policy 23, 545–594.
- Clemens, M., Radelet, S. and Bhavnani R. (2004). Counting chickens when they hatch: The short term effect of aid on growth. Center for Global Development Working Paper 44. Washington, DC: Center for Global Development.
- Easerly, W., Levine, R. and Roodman, D. (2003). New data, new doubts: Revisiting ‘‘Aid, Policies and Growth’’, vol. 26. Washington, DC: Centre for Global Development.
- Farag, M., Nandakumar, A. K., Wallack, S. S., Gaumer, G. and Hodgkin, D. (2009). Does funding from donors displace government spending for health in developing countries? Health Affairs (Millwood) 28, 1045–1055.
- Foster, M. and Leavy, J. (2001). The choice of financial aid instruments. London: Overseas Development Institute.
- Frot, E. and Santiso J. (2010). Crushed aid: Fragmentation in sectoral aid. OECD Development Centre Working Papers 284. Paris: Organisation for Economic Development and Co-operation.
- Gottret, P. and Schieber, G. (2006). Health Financing Revisited – A Practitioner’s Guide. Washington, DC: World Bank.
- Institute of Health Metrics and Evaluation (2010). Financing Global Health 2010: Development assistance and country spending in economic uncertainty. Seattle, WA: IHME.
- Juliet, N. O., Freddie, S. and Okuonzi, S. (2009). Can donor aid for health be effective in a poor country? Assessment of prerequisites for aid effectiveness in Uganda. Pan African Medical Journal 3, 9. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2984282/
- Knack, S. (2012). When do donors trust recipient country system. World Bank Working Paper No. 6019. Washington, DC.
- Knack, S. and Rahman, A. (2007). Donor fragmentation and bureaucratic quality in aid recipients. Journal of Development Economics 83, 176–197.
- Lahiri, S. and Raimondos-Moller, P. (2004). Donor strategy under the fungibility of foreign aid. Economics and Politics 16, 213–231.
- Lu, C., Schneider, M. T., Gubbins, P., et al. (2010). Public financing of health in developing countries: A cross-national systematic analysis. Lancet 375, 1375–1387.
- Martinez A´ lvarez, M. and Acharya A. (2012). Aid-effectiveness in the health sector, Working Paper No. 2012/69. Helsinki: UN_WIDER.
- McCoy, D., Chand, S. and Sridhar, D. (2009). Global health funding: How much, where it comes from and where it goes. Health Policy and Planning 24, 407–417.
- Medlin, C. A., Chowdhury, M., Jamison, D. T. and Measham, A. R. (2006). Improving the health of populations: Lessons of experience. In Jamison, D. T., Breman, A. R., Measham, A. R., et al. (eds.) Disease control priorities in developing countries, 2nd ed., Ch. 8., pp. 161–180. New York: Oxford University Press.
- Minoiu, C. and Reddy, S. G. (2010). Development aid and economic growth: A positive long-run relation. The Quarterly Review of Economics and Finance 50, 27–39.
- Mishra, P. and Newhouse, D. (2007). Health aid and infant mortality. Washington, DC: International Monetary Fund.
- Monkam, N. F. K. (2008). The money-moving syndrome and the effectiveness of foreign aid. PhD Thesis, Georgia State University.
- Mueller, D. H., Lungu, D., Acharya, A. and Palmer, N. (2011). Constraints to implementing the essential health package in Malawi. Public Library of Science One 6, e2071–e2075.
- Nugent, R. A. (2010). Where have all the donors gone? Scarce donor funding for non-communicable diseases. Center for Global Development.
- OECD (2008a). 2008 Survey on monitoring the Paris declaration. Effective aid by 2010? What will it take. Overview, vol. 1. Paris and Washington, DC: Organization for Economic Co-operation and Development.
- OECD (2008b). 2008 Survey on monitoring the Paris declaration: Making aid more effective by 2010. Better aid. Paris: Organization for Economic Co-operation and Development.
- OECD (2013). Available at: https://www.oecd.org/dac/financing-sustainable-development/.
- Pack, H. and Pack, J. R. (1993). Foreign aid and the question of fungibility. Review of Economics and Statistics 75, 258–265.
- Rajan, R. and Subramanian, A. (2008). Aid and growth: What does the cross-country evidence really show? The Review of Economics and Statistics 90, 643–665.
- Ravishankar, N., Gubbins, P., Cooley, R. J., et al. (2009). Financing of global health: Tracking development assistance for health from 1990 to 2007. Lancet 373, 2113–2124.
- Stuckler, D., Basu, S. and McKee, M. (2011). International Monetary Fund and aid displacement. International Journal of Health Services 41, 67–76.
- https://www.cgdev.org/topics/aid_effectiveness Center for Global Development.