In the course of development, few processes are as intertwined with economic growth as human capital accumulation. Schooling makes workers more productive, speeds the development of new technologies, and better equips parents to raise skilled children, all of which promote economic growth. Growth, in turn, incentivizes investment in human capital. Causal links point in every direction, traversing phases of the lifecycle as well as generations.
However, the entangled role of human capital is not limited to aggregate income growth. Education exhibits complex dynamic relationships with several components of wellbeing, including health. For example, education affects health in adulthood; life expectancy affects educational investment in childhood; and the health and education of parents – particularly mothers – affect both outcomes in their children. Just as with income, these relationships are likely to be especially important in developing countries, where levels of both schooling and health are low but have risen rapidly over the past half-century.
This article gives an overview of the current knowledge on the relationships linking health and education in developing countries. To emphasize the dynamic aspects of these relationships, the article will trace them out first within a generation, between childhood and adulthood, and then across generations, from parents to children. It will focus on reduced form evidence of these effects rather than efforts to precisely pin down mechanisms, for two reasons. First, the existing literature focuses on reduced-form evidence. Mechanisms have received some attention, but the evidence comes mainly from rich nations; even that evidence remains sparse.
Second, the reduced-form evidence on dynamic links casts in stark relief the potential joint role of education and health in accounting for the intergenerational persistence of disadvantage. That is to say, the children of unhealthy and uneducated parents grow up to be unhealthy and uneducated parents themselves. Others have proposed similar arguments about the intergenerational dynamics of the relationship between health and socioeconomic status, more broadly construed. But the links between education and health, which typically lie at the crux of these arguments, can by themselves account for the dynamics. Given the current extent of inequalities in income, human capital, and health in developing countries, the links between education and health may prove important in shaping long-term trends in the levels and distributions of both variables.
Associations between health and education are not new, but with such tangled causal pathways, these associations sometimes prove to be uninformative. The recent literature in economics has made its main contribution in causal inference. Analyses of natural experiments and prospective trials have shed new light on long-standing hypotheses. They have also improved our ability to interpret careful associational studies, which are in many cases more generalizable than experimental studies but less internally valid. These advances have been key to identifying both the direction and the timing of effects in the causal system linking education and health. With this better understanding of what matters and when, policymakers will be better equipped to identify opportunities for well-targeted policies.
Mapping The Relationship Between Education And Health
With its numerous pathways, the causal system linking education and health may seem convoluted. However, one can represent it in a simple but informative diagram. Figure 1 traces out the links between education and health, first over the lifecycle and then across generations. Each arrow represents a causal link that has empirical support in the literature. The blue lines signify intragenerational links – in other words, causal links that operate within a single person – whereas the red lines correspond to links that work across generations within a family.
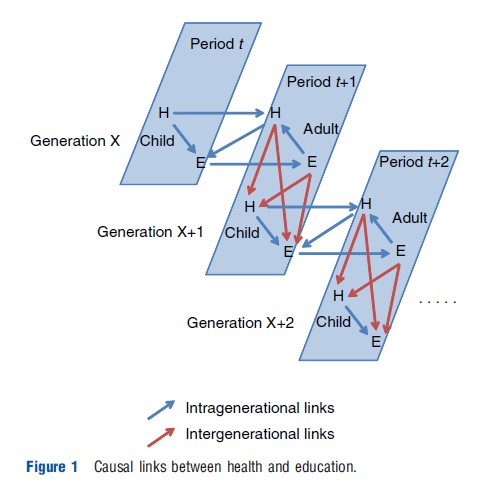
The system lays out a roadmap for the rest of the article. In childhood, good health improves educational outcomes. Additionally, the expectation of good adult health increases schooling investments in childhood. Both health and education persist from childhood to adulthood, at which point education boosts health. But adults are also parents, so their circumstance in middle age spills over onto the next generation. Healthier mothers have healthier and more educated children. Conversely, parental education promotes both the health and the education of the next generation. At this stage, the causal system repeats in the next generation. In the remainder of the article, the focus will be on the subset of the arrows in Figure 1 that connect health and education.
Intragenerational Links
Effects Of Childhood Health On Educational Outcomes
Educational Outcomes In Childhood
The author begins with childhood, where abundant evidence suggests that health affects school enrollment and academic achievement. Health enables children to travel to school, concentrate, and think clearly, all of which may improve educational outcomes. Until recently, the evidence has primarily taken the form of cross-sectional associations between children’s health and their educational outcomes. Many have critiqued these studies for inadequately addressing issues of causality and omitted variables.
Starting in the mid-1990s, a few analyses have made some headway on these issues by focusing on within-family variation. One early study in this literature analyzes data from Ghana and finds, in models with family fixed effects, that shorter siblings start school later than their taller brothers and sisters. A more recent article analyzes twin pairs and sibling sets in Chile, showing that twins or siblings born at higher birth weight perform better on exams. Within-family comparisons of this type eliminate concerns about family level omitted variables, although they leave some concern about how parents allocate scarce resources among children with observably different health.
Analyses of natural experiments in disease eradication, micronutrient supplementation, and health care provision have also made progress on causal identification. One innovative study investigates the eradication of hookworm from the US South in the early twentieth century, finding that areas with higher initial hookworm burdens, and thus likely experienced larger declines in worm prevalence, saw larger in- creases in school enrollment. Another uses contemporary data from Tanzania, focusing on a maternal iodine supplementation program in Tanzania. Drawing on policy variation across time and space, as well as on sibling differences in program exposure, the study finds that in utero exposure to the program increased school participation. In addition to these effects on school participation and enrollment, early-life health boosts test scores. Using data from Chile (and Norway), a recent study takes advantage of the fact that infants born just below the threshold for very low birth weight (VLBW) receive much more care than those born just above. The study documents discontinuities around the VLBW threshold in both infant mortality rates and subsequent test scores, such that infants born below the threshold do better.
In addition to these innovative ways to glean causal effects from observational data, the past decade has seen a series of randomized controlled trials testing the effect of child health on schooling outcomes. Perhaps the best known is a deworming experiment in Busia district, Kenya. Intestinal worms cause anemia and other ailments, which may make children too weak or lethargic to study. After researchers experimentally varied access to deworming medications across 75 primary schools in the district, pupils in treatment schools exhibited significantly lower rates of worm infection, anemia, and school absence, although not test scores. Experimental data on other programs, including one that distributed iron supplements and deworming medication to Indian children and one that distributed protein supplements to Kenyan children, provide corroborating evidence.
Educational Outcomes In Adulthood
The fact that education is relatively fixed by adulthood facilitates the study of its relationship with health. Coupled with retrospective measures of child health, data on adult educational attainment can shed light on the effect of health on education in childhood. For example, just as height and schooling outcomes are associated in children, so too are they related in adults. Adult height positively predicts educational attainment in nationally representative data from Mexico, as well as in data on urban populations in Barbados, Mexico, Cuba, Uruguay, Chile, and Brazil.
In adulthood, too, the results of natural experiments and randomized controlled trials suggest that the associations partly represent an effect of health on education. One noteworthy finding comes from long-term follow-up of the deworming experiment in Kenya. When observed in young adulthood, individuals in the treatment group had stayed enrolled in school longer and performed better on a battery of tests than their counterparts in the control group. However, long-term follow-up of hookworm eradication in the South US gives different results. If one compares birth cohorts born too early to be exposed to eradication to those born later, across areas with differing baseline worm infection prevalence, the results imply significantly positive effects on literacy but not years of schooling.
Several articles have used a similar strategy to estimate the long-term effects of malaria eradication on human capital, with mixed but on net positive results. One study draws on data from the South US, Brazil, Colombia, and Mexico. Here again, significant effects emerge for literacy but not years of schooling, which the author interprets as evidence that eradication made children more productive as students and as child laborers. Separate analyses have applied the same research design to men and women in India, as well as women in Paraguay and Sri Lanka. Although the Indian data show no evidence of positive effects on either literacy or years of schooling, the Paraguayan and Sri Lankan data show the opposite, with large gains in both outcomes.
Effect Of Life Expectancy On Investment In Education
Unlike the effect of child health on education, which is rooted in the technology of skill formation, the effect of life expectancy on human capital investment is, at its core, about optimizing choices by households and individuals. According to the standard reasoning, if an individual expects a longer time horizon to reap the returns to human capital, then that individual will invest more. Analyses of macroeconomic data offer limited support for this hypothesis. Although adult mortality is negatively associated with secondary school enrollment, the relationship is not robust to the inclusion of covariates. However, given the paucity of high-quality data on adult mortality in most countries and the difficulty of assessing causality from cross-country associations, the macroeconomic patterns are suggestive.
Indeed, two microeconomic analyses have yielded convincing evidence that reductions in adult mortality risk increase human capital investment. One novel study uses a period of rapid decline in maternal mortality in Sri Lanka as a natural experiment in adult mortality. Parts of the country with higher baseline maternal mortality rates (and therefore larger subsequent declines in maternal mortality) saw larger increases in female educational attainment. A second study, analyzing the human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS) epidemic in Africa, shows that the subnational regions that were hardest hit by the epidemic have also experienced the largest declines in education.
Effect Of Education On Health In Adulthood
A long-standing literature reports positive associations between education and health in adults in wealthy countries, although the mechanisms linking the two variables are not fully known. To the extent that the association reflects an effect of education on health, important mediators of this effect may include income, working conditions, health-related knowledge, cognitive ability, patience, attitudes toward risk, and cultural capital (especially in interactions with health providers). Similar associations are evident in data from developing countries, although studies are rarer.
Both natural experiments and prospective trials suggest that although education can affect health, such effects may depend on characteristics of the population and the material being taught in school. Several studies use compulsory schooling laws in the US and Europe as instruments for education, with mixed but mildly positive results; some indicate positive effects on health and longevity, whereas others indicate no effect. Unfortunately, no similar studies exist on developing countries.
However, longitudinal follow-up of the recent spate of education-related randomized controlled trials in developing countries has begun to yield useful results on health behavior in young adulthood. One such study analyzes a program in the Dominican Republic that gave teenage boys information about the return to schooling. The information led the boys to stay in school longer, to delay the onset of heavy drinking, and to reduce smoking at the age of 18 years. Across the Atlantic in Africa, another study estimates the effects of a program that sought to provide adolescent girls with both vocational training and information about risky health behaviors. HIV-related knowledge and condom use both increased. However, less promising results have emerged from a Kenyan study on the medium-run impacts of a school subsidy program. Although the program increased schooling for both boys and girls, follow-up data show at best weak impacts on sexual behavior and sexually transmitted disease infection. Together, these studies suggest that keeping boys ‘off the streets’ and equipping girls with health information may be key to any effect of education on health in young adulthood.
Intergenerational Links
Effect Of Parental Education On Child Health
In the context of poor countries, by far the most widely studied education-health association is that between maternal education and child health. Following a canonical study of child mortality in Nigeria in 1979, a large literature has emerged on this topic. The literature bares widespread correlations between maternal education and child health, measured by illness, anthropometry, or death.
Several studies question the extent to which the correlation reflects a causal effect running from maternal education to child health, as opposed to omitted variables. The relationship is not always robust to the inclusion of socioeconomic and community-level covariates, or to the inclusion of a fixed effect for the mother’s sib-ship or for a multifamily household. However, one could interpret many of the socioeconomic and community-level covariates in the literature as mediators rather than confounders, and the inclusion of fixed effects exacerbates problems related to measurement error. The results of the revisionist literature are therefore inconclusive.
Analyses of natural experiments support a causal interpretation. The most compelling evidence comes from the US, where local college openings improve birth weight and gestational age. But some results are also available for developing countries. Among Indonesian women, for example, exposure to a school construction program in childhood reduced mortality rates among their children.
Effect Of Parental Health On Child Education
Parental health also affects children’s schooling outcomes. Two mechanisms stand out in the literature. The first is indirect: Healthier mothers have healthier children, who in turn become better-educated adults. For instance, in utero exposure to the 1918 influenza epidemic decreased educational attainment for the cohort born in 1919 in the US, Brazil, and Taiwan. This effect supports the ‘fetal origins hypothesis,’ which posits that in utero conditions are crucial for the later health and skill development of her child.
The literature also highlights a second mechanism through which parental health affects child education: parental death. Good evidence comes from the HIV/AIDS epidemic, which has orphaned more than 15 million children, some 90% of them in Africa. Across Africa, orphans have lower school enrollment rates than the biological children of their caretakers. Furthermore, in South Africa and Kenya, the timing of parental death is associated with the timing of school dropout. The same is true in Indonesia, where parental deaths typically have little to do to HIV/AIDS. One can thus view the African results as representing a more general effect of losing a parent. Nevertheless, given the scope of the continent’s orphan crisis, the results are most relevant there.
Open Questions
The existing literature fills in many of the links sketched in Figure 1, but open questions remain. For one, the distinction between aggregate and individual educational attainment has received little consideration but is almost certainly relevant for health systems in developing countries. How important is a country’s education system in producing health professionals to support its health system? Additionally, the potential for the backwards intergenerational transmission of health information – from children to parents – remains underexplored. Such information transmission could prove useful in combating the rise of smoking and obesity in poor countries. Concerning intergenerational dynamics in the other direction, from parents to children, the literature would benefit from more focus on how parental behavior reinforces or compensates for exogenous changes in the health environment or educational opportunity. This last line of inquiry would put behavior back in the center of economic research on health and education.
References:
- Alderman, H., Behrman, J. R., Lavy, V. and Menon, R. (2001). Child health and school enrollment: A longitudinal analysis. Journal of Human Resources 36(1), 185–205.
- Almond, D. and Currie, J. (2011). Human capital development before age five. In Ashenfelter, O. and Card, D. (eds.) Handbook of labor economics, vol. 4A, pp 1315–1486. Amsterdam: Elsevier – North Holland.
- Bharadwaj, P., Løken, K. V. and Neilson, C. (2013). Early life health interventions and academic achievement. American Economic Review 103(5), 1862–1891.
- Bleakley, H. (2007). Disease and development: Evidence from hookworm eradication in the American South. Quarterly Journal of Economics 122(1), 73–117.
- Bleakley, H. (2010). Malaria eradication in the Americas: A retrospective analysis of childhood exposure. American Economic Journal: Applied Economics 2(2), 1–45.
- Caldwell, J. C. (1979). Education as a factor in mortality decline an examination of Nigerian data. Population Studies 33(3), 395–413.
- Cleland, J. G. and Van Ginneken, J. K. (1988). Maternal education and child survival in developing countries: The search for pathways of influence. Social Science and Medicine 27(12), 1357–1368.
- Cutler, D. M., Fung, W., Kremer, M., Singhal, M. and Vogl, T. (2010). Early life malaria exposure and adult outcomes: Evidence from malaria eradication in India. American Economic Journal: Applied Economics 2(2), 196–202.
- Cutler, D. M. and Lleras-Muney, A. (2010). Understanding differences in health behaviors by education. Journal of Health Economics 29(1), 1–28.
- Desai, S. and Alva, S. (1998). Maternal education and child health: Is there a strong causal relationship? Demography 35(1), 71–81.
- Field, E., Robles, O. and Torero, M. (2009). Iodine deficiency and schooling attainment in Tanzania. American Economic Journal: Applied Economics 1(4), 140–169.
- Fortson, J. G. (2011). Mortality risk and human capital investment: The impact of HIV/AIDS in sub-Saharan Africa. Review of Economics and Statistics 93(1), 1–15.
- Jayachandran, S. and Lleras-Muney, A. (2009). Life expectancy and human capital investments: Evidence from maternal mortality declines. Quarterly Journal of Economics 124(1), 349–397.
- Lucas, A. M. (2010). Malaria eradication and educational attainment: Evidence from Paraguay and Sri Lanka. American Economic Journal: Applied Economics 2(2), 46–71.
- Miguel, E. and Glewwe, P. (2008). The impact of child health and nutrition on education in less developed countries. In Schultz, T. P. and Strauss, J. A. (eds.) Handbook of development economics, vol. 4, pp 3561–3606. Amsterdam: Elsevier – North Holland.
- Miguel, E. and Kremer, M. (2003). Worms: Identifying impacts on education and health in the presence of treatment externalities. Econometrica 72(1), 159–217.
- Nelson, R. E. (2010). Testing the fetal origins hypothesis in a developing country: Evidence from the 1918 influenza pandemic. Health Economics 19(10), 1181–1192.
- Thomas, D., Strauss, J. and Henriques, M. H. (1991). How does mother’s education affect child height? Journal of Human Resources 26(2), 183–211.