Introduction
The first evidence of mortality being procyclical had been provided by Ogburn and Thomas during the 1920s – procyclical means increasing in good economic times and falling during periods of decline. Additional confirmatory analysis was supplied by Eyer during the 1970s. Nevertheless, until the preceding decade, the conventional wisdom was that health and macroeconomic conditions were positively related. A variety of analyses had been conducted by the strongest adherent of this view, Brenner (1979), who suggested that overall mortality, infant deaths, and fatalities from a variety of sources (including cardiovascular disease, suicide, and homicide) increased during economic downturns, and that morbidity, alcoholism, and admissions to mental hospitals also grew during such periods.
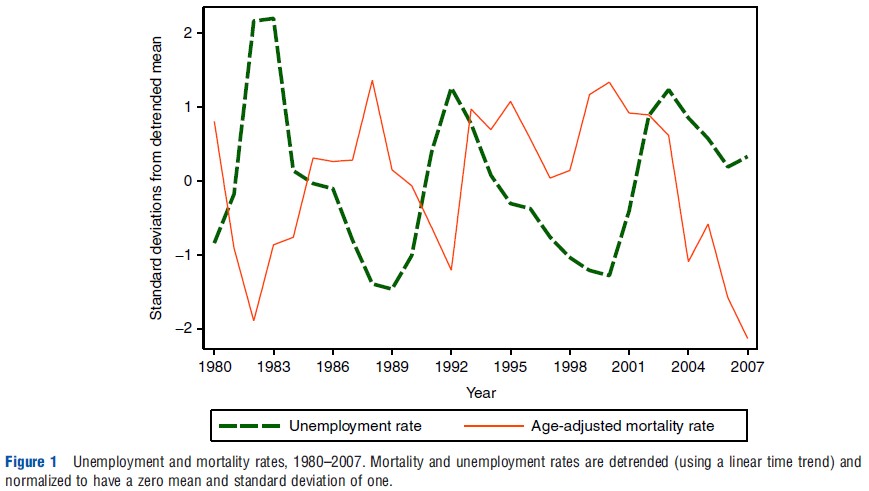
The view that health and economic conditions must be positively related probably rests more on strongly held prior beliefs than convincing evidence. Even a cursory look at the data raises doubts about whether this is necessarily the case. For instance, Figure 1 shows the relationship between detrended age-adjusted total mortality and unemployment rates in the US, from 1980 to 2007 (both transformed to have a mean of zero and a standard deviation of one). The two data series are close to being mirror images of each other. For instance, normalized unemployment rose rapidly during 1980–82, 1989–92, and 2000–04, whereas mortality was declining faster than its long-term trend. Conversely, improvements in economic conditions during 1983–89 and 1992–2000 were accompanied by smaller than usual declines in mortality (or even increases in some years). Such relationships need not be causal but they do suggest that skepticism is warranted with regard to the conventional belief that health improves during good economic times.
Time-Series Analyses
Research conducted before the beginning of the twenty-first century for examining the relationship between macroeconomic conditions and health, typically used a lengthy time series of data aggregated over an entire country. For instance, Brenner’s influential research had utilized data from the US or the UK, covering a four-decade period beginning in the 1930s.
The typical model estimated in these types of analyses is some variation of:
![]()
where H is the health or mortality outcome, E is the proxy for macroeconomic conditions, X is a set of supplementary controls, and e is an error term. More complicated specifications are often estimated including, for example, lags of the macroeconomic variables or detrended values of the dependent and some independent variables. However, this does not change the basic nature of these estimates. The coefficient of key interest y will be biased if cov(Et,εt)≠0, which occurs if there are important uncontrolled for confounding factors. This will frequently be a significant problem because any long time series is likely to have omitted factors that affect health and may be spuriously correlated with economic conditions. For instance, unemployment declined dramatically after the 1930s, when the Great Depression ended, but mortality decreased at the same time due to improvements in nutrition and in the availability of antibiotics. Failure to control for these causes of better health leads to an over-estimate of the detrimental effects of poor macroeconomic conditions.
Presumably because of these issues, time-series studies have arrived at mixed conclusions, with the results being sensitive to the countries, time periods, and proxies for health analyzed. Recent time-series analyses attempt to correct for some inherent in earlier studies, for instance, using statistical rather than ad hoc procedures to model the effect of lags in economic conditions, and correcting for nonstationarity in the data. These innovations do not, however, resolve the basic shortcoming of using a single time series and the results remain ambiguous, although most frequently suggesting that economic downturns are associated with lower mortality.
Estimation Using Pooled Data
One solution to the problem of omitted time-varying confounding factors is to estimate models using pooled data containing time-series information for multiple geographic areas. A key advantage is that, if economic conditions evolve at least somewhat independently (across locations), this geographic heterogeneity can be utilized to control for time-varying confounding factors that have a common influence on health (across locations) at a point in time. An example is the development of widely disseminated new medical technologies for the improvement of health.
These analyses may use aggregate data (such as total or cause-specific mortality rates) or individual-level information, but with the macroeconomic proxies referring to the area and not the person. In the first case, the typical estimation model is some modification of:
![]()
where Yjt is a health outcome or input in location j at time t, E is the proxy for macroeconomic conditions, X indicates supplementary controls, a is a geographic area-specific fixed effect, λ a general time effect, and e is the regression error term. The corresponding specification being used with individual data is:

where i indexes the individual and some of the X variables may be at the person rather locality level.
In eqns [2] and [3], the location-specific ‘fixed effects’ (aj) account for all health determinants that vary across geographic areas but are stable over time. For instance, this could include persistent differences in health behaviors (Victor Fuchs’ provides the classic example of disparities in lifestyles between residents of Nevada and Utah), road conditions (that affect traffic fatalities), or medical facilities (e.g., the presence of tertiary-care hospitals). The time effects (λt) control for health determinants varying over time uniformly across locations. This includes many innovations in medical technologies, as already mentioned, and also other factors such as national trends in eating habits. Factors that vary within locations over time are not accounted for, but this is often, at least partially, remedied by including controls for location-specific time trends.
The macroeconomic effects are then identified by comparing changes in within-locality health, behaviors, or mortality outcomes, as a function of within-locality changes in macroeconomic conditions (controlling for general time effects). This procedure exploits the fact that local economies are less than perfectly correlated. For example, California’s unemployment rate rose much more rapidly from January of 2007 to January of 2010 (from 5.4% to 13.2%) than that of either Texas (from 4.8% to 8.6%) or New York (from 5% to 9.4%).
A potential shortcoming of this procedure is that national changes in macroeconomic conditions are absorbed in the vector of time variables. Thus, the effects of localized rather than national variations in economic performance are identified and the two need not be exactly the same. Some researchers have addressed this issue by using similar estimation techniques but with data pooled across countries (rather than regions within countries), although this raises questions about generalizability of the results because institutions exhibit substantial cross-national variation.
Researchers have most frequently used unemployment rates as the macroeconomic indicator, although other measures (such as deviations of gross domestic product from trend or the percentage of the prime-age population employed) have sometimes been utilized. However, it is important to realize that these estimates do not measure the effects of an individual becoming unemployed or changing labor market status per se – which is often the focus of epidemiological studies – but instead, these rates are used as a broader marker of economic conditions. It is possible for average health to improve during economic downturns, even when there are negative health effects on those who lose jobs.
Supplementary controls vary but frequently include age, education, and race/ethnicity, with more detailed sets of regressors being generally incorporated into models that are estimated using individual-level (rather than aggregated) data. Incomes are often also included as right-hand side variables but the results must be interpreted with care, because a portion of the macroeconomic effects may operate through changes in incomes. Similar issues arise when controlling for health behaviors (like smoking or physical activity) or medical care utilization, because these may be correlated with health, but partially determined by economic conditions. A variety of methods have been used to examine dynamics of the adjustment process such as, for example, adding lags of the macroeconomic proxies to the model and simulating the effects of either temporary or lasting changes in economic conditions.
Mortality Is Procyclical
Research using the longitudinal methods just described in Section Estimation Using Pooled Data has most commonly examined mortality rates. Deaths are of obvious importance because they constitute the most severe negative health shock. They are also objective and well-measured indicators of health that do not require access to the medical system for diagnosis. However, the cause of death may be measured with error, and fatalities do not capture the effects of some health problems (e.g., arthritis) that are either unrelated or only weakly related to mortality.
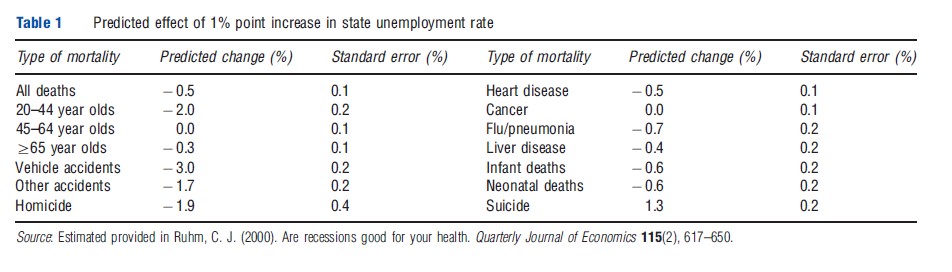
In a particularly influential study published in the May 2000 issue of the Quarterly Journal of Economics, Ruhm had examined how total, age-specific, and cause-specific mortality varied with economic conditions (primarily proxied by unemployment rates) for the 50 US states and District of Columbia over the period 1972–91. Key results, summarized in Table 1, indicate that a one percentage point increase in state unemployment rates was predicted to reduce the total fatality rate by 0.5%, corresponding an unemployment elasticity of mortality equal to 0.04. The strongest responses were for traffic deaths, other accidents, and homicides – declining by 3.0%, 1.7%, and 1.9%, respectively – but significant reduction are also estimated to occur for deaths from cardiovascular disease (0.5%), influenza or pneumonia (0.7%), and liver ailments (0.4%). Infant and neonatal mortality were also expected to fall but there was no change found for cancer deaths, whereas suicides were estimated to increase. Interestingly, although the strongest effects had occurred for relatively young adults (where mortality is predicted to fall by 2.0%), substantial reductions were also predicted for senior citizens, who rarely worked.
Following the publication of Ruhm’s article, researchers have used similar methods to examine how economic conditions are related to mortality in various countries and regions of the world. These analyses include studies of 16 German states between 1980 and 2000, 50 Spanish provinces from 1980 to 1997, 96 French departments from 1982 to 2002, 13 EU nations from 1977 to 1996, and 23 Organization for Economic Co-operation and Development (OECD) countries from 1960 to 1997. Virtually, in all of these studies, it has been found that total mortality and motor vehicle fatalities decline when economic conditions worsen, with the estimated elasticities being generally similar in size or larger than those found in the US.
Deaths from cardiovascular disease are also found to fall as the macroeconomy weakens, in most studies examining them, and a procyclical pattern of deaths from influenza or pneumonia is also generally obtained. In contrast, as in the US, cancer fatalities are generally (but not always) unrelated to the state of the economy. These results are plausible. For example, it seems likely that deaths from coronary heart disease will induce more responsive changes in modifiable health behaviors and environmental risks than cancer fatalities. Results have been more mixed when considering mortality due to liver disease, suicide, or homicide – with predicted increases when the economy strengthens in some analyses and decreases in others.
There is some indication that macroeconomic conditions have weaker effects on mortality in countries with strong social safety nets. The results for infant and neonatal mortality also appear to differ across institutional environments, with evidence of strong procyclical variations being obtained for the US, but not for Germany or when OECD countries are the unit of analysis.
Although most research has been for the US or Western European nations, this is starting to change. Recent studies have examined data from eight Pacific Asian nations during 1976–2003 and from 32 Mexican states between 1993 and 2004. The results from Asia largely mimic those obtained for the US, with the prediction of a substantial procyclical variation for total mortality and deaths from traffic accidents or cardiovascular disease, but with (insignificant) countercyclical variation for suicides. The results for Mexico are particularly interesting. The overall findings again indicate that deaths from all causes and most specific causes of mortality (including cancer deaths but not suicides) decline when the economy weakens. However, these patterns pertain to wealthy states only, with mortality in poor states exhibiting a countercyclical fluctuation. Given the wide income disparities between rich and poor Mexican states, such results are consistent with temporary improvements in macroeconomic conditions worsening average health in wealthy areas but improving it in poor ones. The latter finding is anticipated because the marginal benefits of income are likely to be exceedingly high when incomes are very low.
Other Measures Of Health
There has been less study of how macroeconomic conditions are related to other measures of health, largely because data useful for examining this issue are harder to come by. Using information from the 1972 to 1981 waves of the National Health Interview Survey (NHIS), one study had found that adult morbidity declined when economic conditions weakened, with larger reductions in acute than in chronic medical conditions. Restricted-activity and bed-days also became less common and there were relatively large reductions in the prevalence of ischemic heart disease and certain back problems. However, this study has provided evidence that nonpsychotic mental disorders increased during such periods which, when combined with prior findings of a procyclical variation in suicides, suggests that mental health may decline during periods of economic deterioration despite the improvement of physical health.
Consistent with the possibility that individuals would become (physically) ‘healthier but not happier’ during downturns, a study of more recent (1997–2001) NHIS data revealed that the mental health of African-American and less-educated males declined when the economy weakened. Another analyses of 10 years of data (1984–93) from the Panel Study of Income Dynamics had revealed that average self-assessed overall health status fell when local unemployment rates increased and that these effects were largely driven by psychological rather than physical factors.
Changes In Behaviors And Use Of Medical Care
There is improvement of physical health during bad economic times because healthier lifestyles are adopted by individuals. Alcohol sales and drunk driving vary procyclically and most research has also indicated that alcohol consumption, dependence, and heavy drinking decline when the economy weakens. However, the evidence from individual-level data is more ambiguous, with one study obtaining the contradictory result that binge drinking increases, whereas overall and heavy drinking fall; another finds an increase in alcohol use among teenagers during such periods. Finally, data for Finland provides some evidence of a countercyclical variation in certain categories of alcohol-related deaths between 1975 and 2001; however, the reverse pattern is observed for the period surrounding the extreme downturn of the 1990s and there is again evidence obtained for a procyclical pattern of overall drinking.
Other behaviors also become healthier when the economy weakens. Analysis of data of the Behavior Risk Factor Surveillance System (BRFSS) from 1987 to 2000 has indicated that severe obesity, tobacco use, and multiple behavioral risk factors decline in bad economic times, whereas physical exercise increases. Further evidence of a procyclical variation of obesity has been obtained from an analysis of the BRFSS during 1984–2002 and in smoking and physical inactivity from a study of 1976–2001 data from the NHIS. There is also an indication that diets become healthier during bad times, although relevant data are inadequate to state this with confidence. Also, less alcohol is consumed by pregnant women during such periods and their sleeping span (which has beneficial impacts on health) increases. However, the lifestyle changes need not be uniform across countries or population groups. For instance, there is some evidence of a countercyclical variation in obesity for African-American men and possibly for Finnish adults.
Better health during downturns is not the result of greater use of medical care – the utilization of most (but not all) types of medical services declines in such periods. Specifically, there is a reduction in routine medical checkups and doctor visits, screening tests, and hospital episodes. This is probably partially due to reductions in employer-provided health insurance, but may also reflect improvements in health itself. Nor are these effects uniform. For instance, there is evidence that advanced treatments for heart disease (like coronary bypass and angioplasty) become more common in bad times and that pregnant women receive earlier and more frequent prenatal care in such periods.
Sources Of Countercyclical Variations In Health
As already been mentioned, one reason for health improvement during bad economic times is the adoption of healthier lifestyles. Some of this change probably occurs because of increased availability of nonwork time during such periods, which is important because activities such as exercising and preparing meals at home are relatively time intensive. Consistent with this is the evidence that higher time prices are correlated with increases in tobacco use and reductions in exercise and socializing. However, there are other reasons why health is being countercyclical. For instance, hazardous working conditions, physical exertion of employment, and job-related stress may all increase during economic expansions, as working hours and pace of jobs rise. Moreover, employment growth during such periods is particularly large in the construction and manufacturing sectors, which have relatively high rates of work-related accidents, and these risks are amplified by the relatively higher presence of inexperienced workers. Incomes also rise during economic booms, which help to explain the rise in risky activities such as drinking and smoking. However, the direct effect of income as estimated for mortality and other health behaviors is often mixed, with a protective impact being often observed for morbidity and functional limitations.
Health may also decline when the economy improves because the former is an input for temporary increases in the output of the latter. As already been mentioned, many individuals will be required to work harder or longer in expansions, and joint products of economic activity – like pollution, driving, and traffic congestion – present further health risks. These latter effects are not limited to persons directly involved in the labor market conditions, but instead, they may frequently be concentrated among those with health vulnerabilities, like senior citizens or infants. Such groups may also be strongly though indirectly affected when care-giving behavior among prime age individuals is modified by increases in the workhours of their employment or by their geographic migration in search of better employment opportunities.
Relatively strong procyclical fluctuations in mortality for senior citizens were documented and discussed in Section Mortality is Procyclical (Table 1), providing evidence of such indirect effects. An in-depth analysis of this same issue has recently been conducted by Miller et al. (2009) using data from the Centers for Disease Control and Prevention Multiple Cause of Death Files covering 1978–2004. They have confirmed that there is a strong pattern of procyclical mortality for young adults (18–35 year olds), but have also shown that death rates rise strongly in good times for children (0–17 year olds) and senior citizens, particularly those aged 80 years and above. In contrast, the fatality rates of 35–54 year olds are little affected by macroeconomic conditions. They emphasize the role of factors other than ‘own work behavior’ (like changes in pollution or the quantity, quality, and nature of health care) as potential mechanisms for explaining these results.
Caveats And Uncertainties
Two important caveats should be kept in mind when interpreting the preceding discussion. First, that the macroeconomic fluctuations so discussed refer to transitory rather than permanent changes in economic conditions. Evidence of physical health improving during transitory downturns should not be taken to imply that permanent economic progress has negative effects. A key distinction is that temporary increases in output can only be obtained by using inputs (including health) more intensively given existing technologies. In contrast, permanent growth results from a combination of technological improvements and expansions in the capital stock (including human capital) that would generally result in higher levels of both economic output and health. For example, there is clear evidence that economic development among previously impoverished countries yields health improvements (although there is less indication of corresponding effects among already industrialized nations).
That said, additional study is needed to determine how long economic growth must be sustained before the initial negative consequences for health turn positive. Previous research permitting such dynamics has generally found that the effects of sustained changes in economic conditions usually accumulate for at least 1 or 2 years, consistent with models where flows of health capital gradually affect overall levels of health, resulting in larger increases in the medium term than initially. Attenuation in the predicted health effects of longer lasting changes in the macroeconomy is observed for some outcomes or studies, but not for others and further investigation of this topic is needed.
Several other uncertainties could be resolved by further research. Generally, one has more understanding of how the macroeconomy affects health than of the mechanisms for these effects. It is particularly important to obtain estimates of the role of environmental risks and other factors (like care giving) that are not directly related to an individual’s own labor market experience but may influence health. Data limitations also make it harder to study consequences for mental health and morbidity than it does for mortality, although progress in these areas is being made. How the health effects of macroeconomic conditions vary across institutional environments and levels of economic development are also begun to be learnt, but additional study is required.
Bibliography:
- Brenner, M. H. (1979). Mortality and the national economy. Lancet 314, 568–573.
- Miller, D. L., Page, M. E., Stevens, A. H. and Filipski, M. (2009). Why are recessions good for health. American Economic Review 99, 122–127.
- Charles, K. K. and DeCicca, P. (2008). Local labor market fluctuations and health: Is there a connection and for whom? Journal of Health Economics 27, 1532–1550.
- Dehejia, R. and Lleras-Muney, A. (2004). Booms, busts, and babies’ health. Quarterly Journal of Economics 119, 1091–1130.
- Eyer, J. (1977). Prosperity as a cause of death. International Journal of Health Services 7, 125–150.
- Fuchs, V. (2011). Who shall live? Health, economics and social choice (expanded second edition). Singapore: World Scientific Publishing.
- Gerdtham, U. G. and Ruhm, C. J. (2006). Deaths rise in good economic times: Evidence from the OECD. Economics and Human Biology 43, 298–316.
- Granados, J. A. T. (2005). Increasing mortality during the expansions of the US economy, 1900–1996. International Journal of Epidemiology 34, 1194–1202.
- Gravelle, H. S. E., Hutchinson, G. and Stern, J. (1981). Mortality and unemployment: A critique of Brenner’s time-series analysis. Lancet 318, 675–679.
- Ogburn, W. F. and Thomas, D. S. (1922). The influence of the business cycle on certain social conditions. Journal of the American Statistical Association 18, 324–340.
- Ruhm, C. J. (2000). Are recessions good for your health? Quarterly Journal of Economics 115(2), 617–650.
- Ruhm, C. J. (2005). Healthy living in hard times. Journal of Health Economics 24, 341–363.
- Ruhm, C. J. (2007). A healthy economy can break your heart. Demography 44, 829–848.
- Ruhm, C. J. (2008). Macroeconomic conditions, health and government policy. In Schoeni, R. F., House, J. S., Kaplan, G. A. and Pollack, H. (eds.) Making Americans healthier: Social and economic policy as health policy: Rethinking America’s approach to improving health, pp 173–200. New York: Russell Sage Foundation.
- Stuckler, D., Basu, S., Suhrcke, M., Coutts, A. and McKee, M. (2009). The public health effect of economic crises and alternative policy responses in Europe: An empirical analysis. Lancet 374, 315–323.